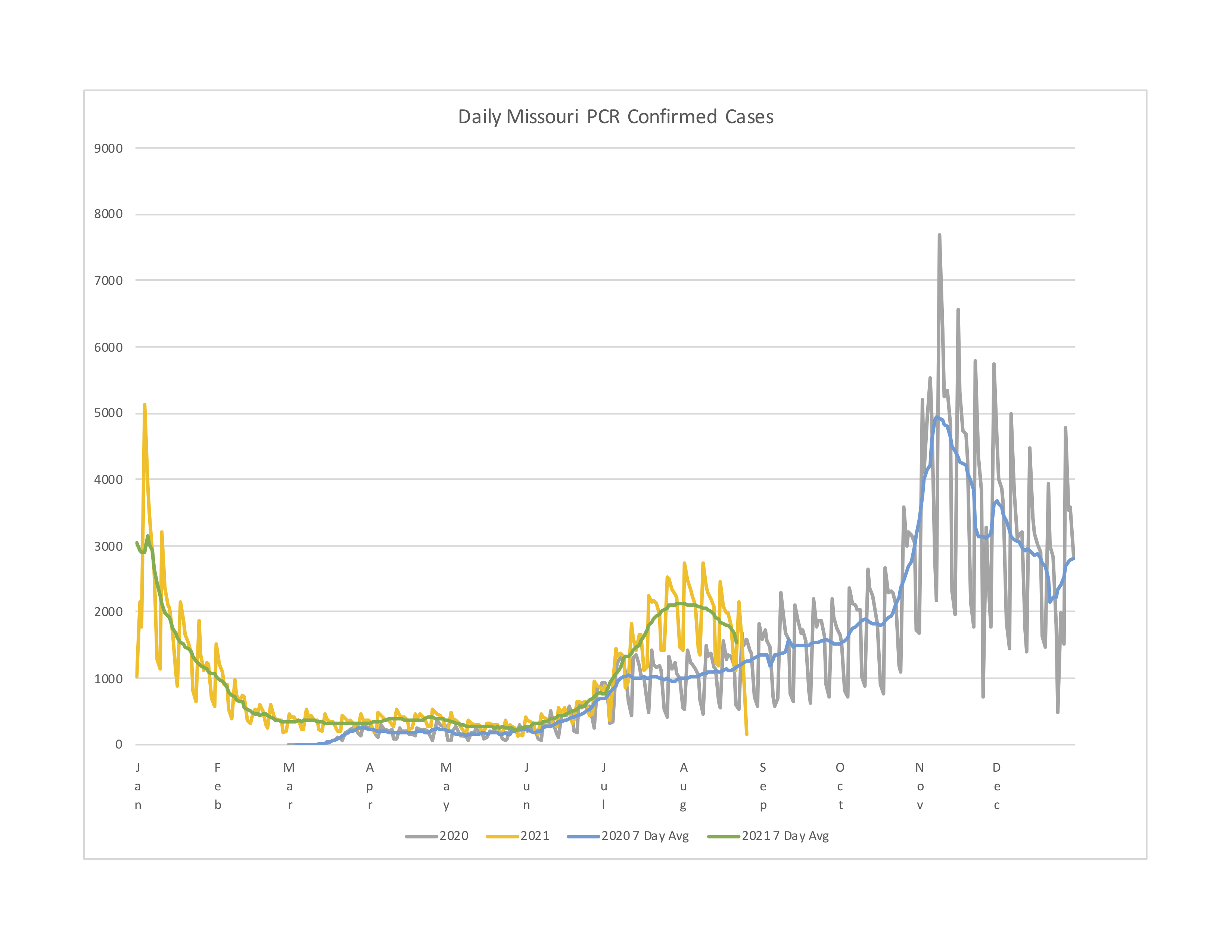
I plotted COVID cases and deaths here in Missouri with year on top of year which I think is important with a seasonal virus. While there were divergences between cases and deaths in 2020, 2021 they look pretty lock step taking into account the slight delay from cases to deaths.
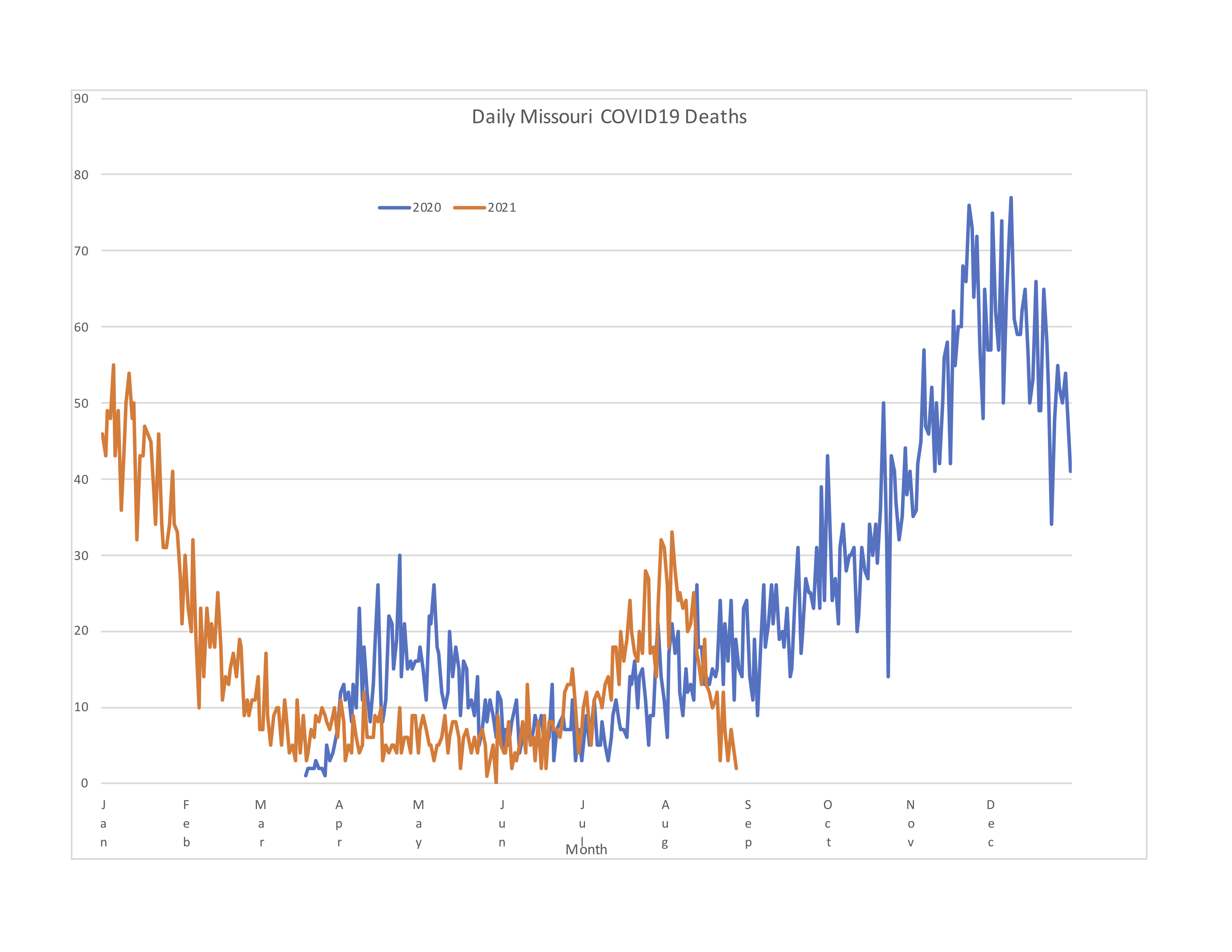
My biggest takeaway looking at the death chart is that while happy days may not be here again, happier days are – as long as the drop isn’t due to delays in death reporting. The fact that cases and deaths have been dropping essentially for the month of August while last year they kept rising is a good sign, a sign that between vaccinations and infections the virus is running out of susceptible people to infect. I would be concerned that if the cases chart is a more accurate indication of seasonality, we might still have a fourth wave coming in November (again).
Another take away is since we’ve been through three waves in Missouri, we have achieved “herd immunity” three times already, IOW R (reproduction number) has been above 1 three times and below 1 three times (don’t even get me started on R naught for a seasonal virus). I think we are headed to COVID becoming an endemic minor childhood disease but we still have some rough times ahead to get there in the year to come. If you have not gotten infected or vaccinated yet, your choice is either to go through an infection vaccinated or unvaccinated, and I’m going to suggest vaccinated is the better way to go. COVID zero is a pipe dream, COVID as just another viral infection amongst others is the reality.
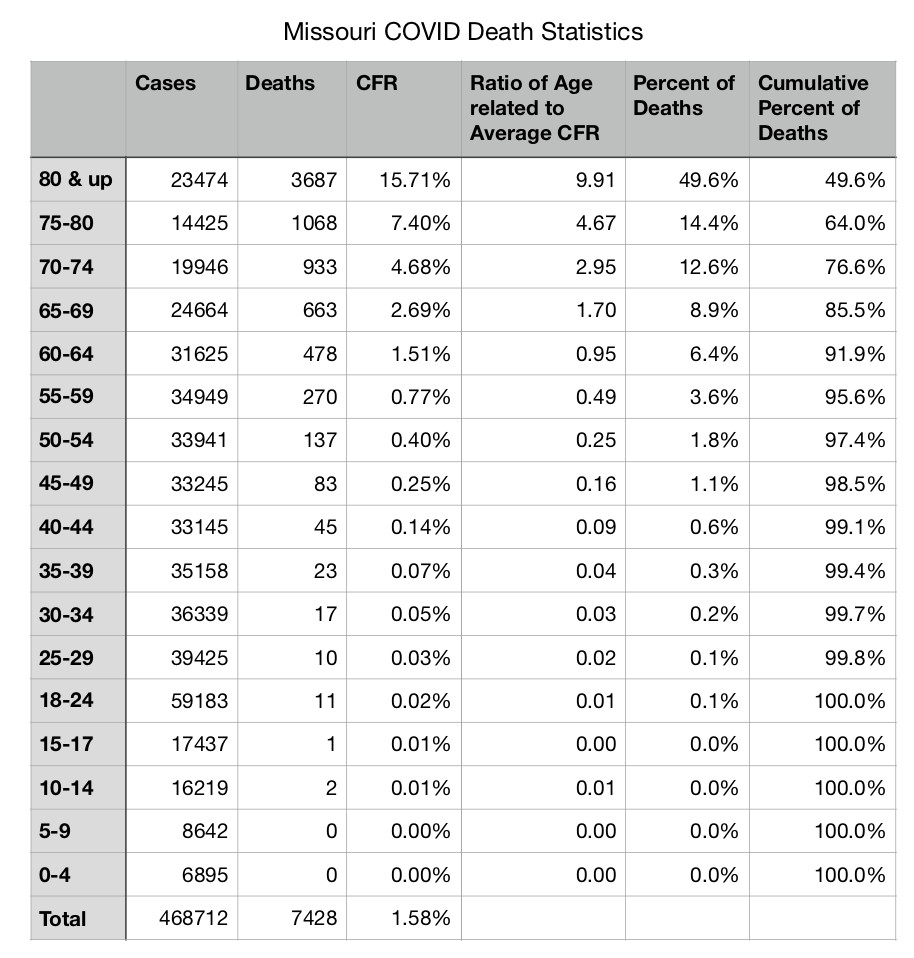
Clearly Delta is more infectious since the late summer surge was greater in 2021 than 2020 despite the fewer susceptible people more people were infected and died. The media keep saying the hospitals and ICUs are as full right now as during the peak last Nov and Dec last year, yet the death rate of the most recent peak is roughly a third what is was then so I have to wonder what is really going on. Are we hospitalizing more for treatment, or are we doing that much better keeping hospitalizations advancing to deaths? Or is the media just being negative and sensationalist? The answer is left as an excercise for the reader.